Article Text

Abstract
Aim The study aimed to assess job demands at the patient’s bedside and to evaluate the contribution of this central workplace to the stress and satisfaction of nurses.
Design In this cross-sectional survey study, a questionnaire was compiled and all registered nurses from intensive, general and intermediate care wards at a large German hospital were invited to participate.
Methods The questionnaire used a list of care activities to assess nurses' workload at the patient’s bed. The German Copenhagen Psychosocial Questionnaire and an adapted version of the German Perceived Stress Scale were used to measure nurses’ stress and burn-out, and single items to assess health status, organisational commitment, job satisfaction, and satisfaction with the quality of care. The questionnaire was returned by 389 nurses.
Results Expected correlations of workload at the patient’s bed with stress, burn-out and satisfaction of the nurses were shown. A moderating effect of organisational commitment was non-existent but was shown for the self-assessed health on the correlation between workload and satisfaction with the quality of care. Organisational commitment correlated negatively with stress and burn-out and positively with satisfaction. The study provides evidence that rates of burn-out and stress do not differ based on the work area of nurses. Because job demands at the patient’s bed correlated with all outcomes, measures to improve this specific workspace are sensible.
- Nurses
- STRESS
- Burnout, Professional
- Healthcare quality improvement
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In Germany, there is a shortage of trained nursing staff and nurses experience a high physical and mental burden while working in direct patient care, which could be counteracted by improving the working conditions.
WHAT THIS STUDY ADDS
The results indicate that the job demands while working at the patient’s bed correlate with nurses’ strain, well-being and satisfaction, occurring equally across work areas in the hospital.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
As work at the patient’s bedside was shown to correlate with nurses’ stress and satisfaction measures to improve this workplace should be taken, but further research is needed to generalise the findings across clinics.
As organisational commitment was shown to be directly correlated to nurses’ outcome variables, this indicates the chance for organisational management at clinics to actively engage in improving nurses’ work environments, by for example strengthening occupational health management.
The moderating effect of self-assessed health that only occurred in connection with satisfaction with the quality of care, should lead to further research to better understand this relation.
Introduction
The appropriate functioning of health systems during the COVID-19 pandemic has proven the relevance of the nursing profession. However, even before the pandemic, the working conditions of nurses have been a concern.1 Despite being an indispensable part of healthcare, there exists a lack of trained nursing staff, historically referred to in Germany as the ‘nursing crisis’.2 3 For years, the number of nurses leaving the system has been greater than the number of trained new entrants.4 Comparing European countries, Germany has performed below average in the nurse-to-bed ratio.5 In addition, the low median income in the nursing sector,2 6 health conditions and job satisfaction are discussed as being an impetus for the nursing crisis.4 5 In improving the working conditions and in counteracting this crisis, concentrating on strategies to relieve the workload in the nursing profession is necessary.1
Background
Overall, the nursing profession is characterised by a high physical and mental burden.7–9 Nursing workload is defined as ‘the amount of time and physical and/or cognitive effort required to accomplish direct patient care, indirect patient care and non-patient care activities’.10 Resulting of the complex demands and high workload, nurses experience strain in the form of physical discomfort and stress.7 The greatest stressors for nurses are the workload and the emotional confrontation with death and dying.11 12 Inadequate preparation for treatment, management of patients and relatives, and absence of scope or social support are also mentioned.11 13 Especially in social and care professions a specific long-term consequence of stress at work is burn-out.14 The reported global prevalence among nurses is 11% but varies significantly between regions, specialties and burn-out measures used.15 16 Burn-out is associated with an increased likelihood of changing professions,17 decreased patient and job satisfaction,18 19 and reduced quality of care.20 Thus, considering nurses’ job satisfaction is crucial because it is influenced by workload, direct patient care and organisational culture.12 21 Additionally, nurses’ dissatisfaction is a primary reason for changing careers.4
This study aims to assess the job demands of nurses while working at the patient’s bed and related psychosocial factors, based on the job demands-resources model (JD-R).22 We expect job demands while working at the patient’s bed to correlate with strain and satisfaction of nurses as this was found in comparable studies for general job demands (h1: job demands are positively related to strains; h2: job demands are negatively related to nurses’ satisfaction).23–25 Organisational commitment is included to explore its influence on the correlation between job demands and strain (h3. perceived organisational commitment reduces the correlation between job demands and strains). Research in a similar population found a buffering role of organisational resources, as assumed in the JD-R.26 We examine whether organisational commitment is related to nurses’ satisfaction, as comparable studies show the relation between organisational resources and nurses’ satisfaction and their ratings of the quality of care (h4: perceived organisational commitment is positively related to nurses’ satisfaction).18 27 Additionally, we investigate whether there are differences among specific work areas because results on how and whether specific work areas differ in their burden for nurses have been inconsistent.28
Method
Study design
To attain a high response rate and to enable comparison within a larger project, we conducted a survey study. Results are correlational and no causal conclusions can be drawn. This cross-sectional study follows the Consensus-Based Checklist for Reporting of Survey Studies, which is included as an additional file.29
Data collection
Pretest
A pretest of the questionnaire was conducted from 10 March 2020 to 24 March 2020 to test readability, structure and acceptance. Nurses (N=115) of two randomly selected wards (intensive care: n=81; neurology: n=34) were invited and n=31 (response rate 27%) questionnaires were returned (cf. online supplemental appendix 1). No major concerns were reported.
Supplemental material
Main survey
The questionnaire was compiled by an interprofessional expert group, including researchers and representatives from the nursing staff. To ensure access for all participants, the questionnaire was distributed as a paper-and-pencil version on the participating wards. The overall questionnaire consisted of 52 items. Items for sample description were age, gender and work area.
Job demands at the bedside were recorded with 16 tasks, rated for subjective workload and expenditure of time, resulting in 32 questions. Answers were provided on a five-point Likert scale with the additional option ‘cannot be answered’.
Stress at work was assessed with an adapted version of the German Perceived Stress Scale (PSS) using 10 items. The PSS measures the degree to which situations in an individual’s life are perceived as unpredictable, uncontrollable or stressful over the past month.30 31 Good psychometric properties were demonstrated for the German version.31 Because the PSS measures perceived stress in life in general, four items were adapted: ‘in their life’ was replaced by ‘at work’. In addition, two items were adjusted to increase comprehensibility.
To assess burn-out, the Burn-out Symptoms scale of the German Copenhagen Psychosocial Questionnaire (COPSOQ) was used.32 For the Burn-out Symptoms scale, comprising six items, good internal consistency, high generalisability and construct validity have been shown.32 33
The Burn-out Symptoms and the adapted PSS were answered on a five-point Likert scale. The original German PSS uses a different verbalisation of the scale levels, but for consistency, the verbalisation of the COPSOQ was adopted.
The item targeting organisational commitment was based on the concept of organisational support, which describes ‘employees’ general belief that their work organisation values their contribution and cares about their well-being’.34 To fit the study context, it was recorded as ‘organisational commitment of the clinic to reduce the burden in care’ as a single item. General job satisfaction, satisfaction with the quality of care and general health status were also single items. All single items were answered on a 10-point rating scale.
Sample
Included in the study were all employed nurses, full time and part time, at the hospital from intensive, general and intermediate care wards (N=1124). Excluded from participation were nurses from paediatric wards, day clinics, and polyclinics and nurses in training due to comparability reasons. Wards participating in the pretest (N=115) were not included in the main survey because of the short period between the surveys. Participation was voluntary. Since the sample size was tied to the number of participating nursing staff at the hospital, the required sample size was not planned, that is, convenience sampling was used.
Survey administration
The questionnaire was in German (cf. online supplemental material 1) and took approximately 10 min to be completed. To create and automatically read out the questionnaire EvaSys (V.8.0, 2019, 35, Lüneburg, Germany) was used.35 The survey was announced via email and on notice boards. The survey period was from 20 May 2020 to 8 June 2020.
Supplemental material
Participants were informed about background, aims, a contact person and that participation was voluntary and anonymous. Information on the survey period and submission procedure was displayed. For the latter, locked mailboxes were available.
Patient and public involvement statement
Patients and public were not involved in this research. A nursing staff representative was part of the interprofessional expert group developing the questionnaire.
Data analysis
Statistical evaluation was conducted using RStudio (V.1.2.5033, 2016, Boston, Massachusetts, USA).36 For the analyses, inverted items were recoded and records with missing values were removed using row-by-row exclusion. To limit the loss of data, only scales relevant to the respective analyses were filtered using line-by-line exclusion. To ensure the quality of the questionnaire, we recalculated the internal consistency of the scales. Based on prior inconsistent findings (cf. Background), we analysed whether a multilevel model that considers the work area would be appropriate. If this was not the case, multiple regression was calculated. The power of the effects found was determined post hoc using G*Power (V.3.1.9.4, Düsseldorf, Germany).37 38 Assumptions were tested for multiple regressions and multilevel modelling.
The outcome variables were workload, burn-out, job satisfaction and satisfaction with the quality of care. In multiple regressions and multilevel modelling, predictors were added using stepwise inclusion: Subjective workload was included first as the most important predictor following the JD-R. Next, organisational commitment was added as a resource, and subsequently, the variable health status was added. The latter was considered in the exploratory data analysis. To achieve a concise description, the second and third steps of the hierarchical models are reported. For full hierarchical models, see online supplemental material 1.
Results
Descriptive results
Sample
A total of 389 questionnaires were returned, resulting in a response rate of approximately 35% (calculated by dividing the number of returned questionnaires by the number of nurses invited to participate). Datasets in which entire scales were not answered were excluded (n=15), resulting in a sample size for data analysis of n=368. For demographics, see online supplemental appendix 1. For testing the hypotheses and to create a correlation matrix, we created a dataset using z-standardisation and listwise exclusion so that a scope of n=321 remained (cf. online supplemental appendix 2).
Item analysis
All available data points were used to calculate internal consistency, with 5% missing values. The answer option ‘not applicable’ accounted for 27% of the missing values. The scales used had good to very good internal consistency overall (α=0.75–0.91).
Descriptive data
The scales Subjective Workload, Adjusted PSS and Burn-out Symptoms, for which the scale mean was used, were approximately normally distributed. Regarding the single items, the items on satisfaction and health status were somewhat left-skewed. The distribution of the item on organisational commitment indicated a possible floor effect.
Statistical analysis
Stress
In analysing stress as an outcome variable, the inclusion of random intercepts SD=0.12, 95% CI (0.03 to 0.52), χ²(1)=1.32, p=0.25 of the work areas did not lead to a significant improvement. Therefore, multiple regression was calculated to determine the relationship between stress and subjective workload. The model with subjective workload and organisational commitment had a test statistic of F(3,317)=33.1, p<0.001, R²=0.24 and a post-hoc power of 1. The assumptions were tested and no deviations were found. Multiple regression showed a significant positive correlation between subjective workload with stress. Thus, a higher workload level is associated with higher stress in nurses. The interaction of the predictors was non-significant, indicating no buffering effect of organisational commitment on the relationship between stress and burn-out. Additionally, there was a significant negative correlation between organisational commitment and stress, indicating that a higher commitment of the clinic is associated with lower levels of stress (cf. table 1 and online supplemental appendix 3).
Results of multiple regression with stress as outcome variable (n=321)
Burn-out
Using the aforementioned procedure, multiple regression with burn-out as the criterion was also calculated because of a non-significant model improvement through the inclusion of random intercepts SD=0.01, 95% CI (0.11 to 0.12), χ2(1)=0.001, p=0.96. Assumptions were also tested, and no problems were recorded. The model with the predictors subjective workload and organisational commitment showed a test statistic of F(3317)=38.92, p<0.001, a variance explanation of R²=0.27, and a power of 1. Burn-out correlated significantly positively with subjective workload and negatively with organisational commitment (cf. table 2 and online supplemental appendix 4). The interaction of the predictors was non-significant. Thus, the results for burn-out are the same as those for stress.
Results of multiple regression with burn-out symptoms as outcome variable (n=321)
Job satisfaction
Regarding job satisfaction as a criterion, there was also no improvement in the model through the inclusion of random intercepts SD=0.00, 95% CI (0.00 to 0.00), χ2(1)=0, p=0.99. The requirements for multiple regression were fulfilled. The previously described predictor constellation showed a variance explanation of R²=0.20 with F(3317)=26.82, p<0.001 and a power of 1. A significant negative correlation with subjective workload was found, indicating that a higher workload is associated with decreased job satisfaction. Organisational commitment correlated positively with job satisfaction, indicating that the commitment of the clinic is associated with higher satisfaction of nurses (cf. table 3 and online supplemental appendix 5).
Results of multiple regression with job satisfaction as outcome variable (n=321)
Satisfaction with the quality of care
Regarding satisfaction with the quality of care, the inclusion of random intercepts SD=0.14, 95% CI (0.04 to 0.45), χ²(1)=3.00, p=0.08 showed almost no model improvement. However, because the Akaike information criterion had decreased from 915.41 to 914.41, the subjective workload was used as a predictor of satisfaction with the quality of care to check again whether random intercepts improved the model. This was the case with SD=0.16, 95% CI (0.06 to 0.47), χ²(1)=4.95, p=0.03. The inclusion of random slopes, SD=0.11, 95% CI (0.03 to 0.41), χ2 (2)=3.37, p=0.19, showed no significant model improvement. Therefore, in the next step, the predictor organisational commitment was included in the model with only random intercepts. The inclusion of this predictor led to a significant model improvement, with χ²(2)=48.49, p<0.001. The model explained a total of 21% variance (RGLMM(c)²=0.21), of which the predictors explained 17% variance (RGLMM(m)²=0.17).39 The post-hoc power was 1. The assumptions for the multilevel model could be fulfilled. Significant correlations were found to be negative for subjective workload and positive for organisational commitment (cf. table 4 and Online supplemental appendix 6). Thus, the results for satisfaction with the quality of care are the same as the results for job satisfaction.
Results of multilevel model with satisfaction with the quality of care as outcome variable and random Intercepts based on work areas (n=321)
Explorative findings
As part of an exploratory analysis, the variable health status was included in each of the listed analyses (cf. data analysis). No hypotheses were proposed regarding this variable because it can be classified either as a personal resource40 or an outcome variable.32 However, using the JD-R as the theoretical background of this study, this variable was included as a resource in the exploratory analysis. Assumptions on the appropriateness of the procedures were tested individually and could be fulfilled. The inclusion of health status led to a significant model improvement for all outcomes (p<0.001). The significant correlations between workload, organisational commitment and the outcome variables described previously held when health status was included. In addition, the variable showed significant correlations of p<0.001 with all outcome variables.
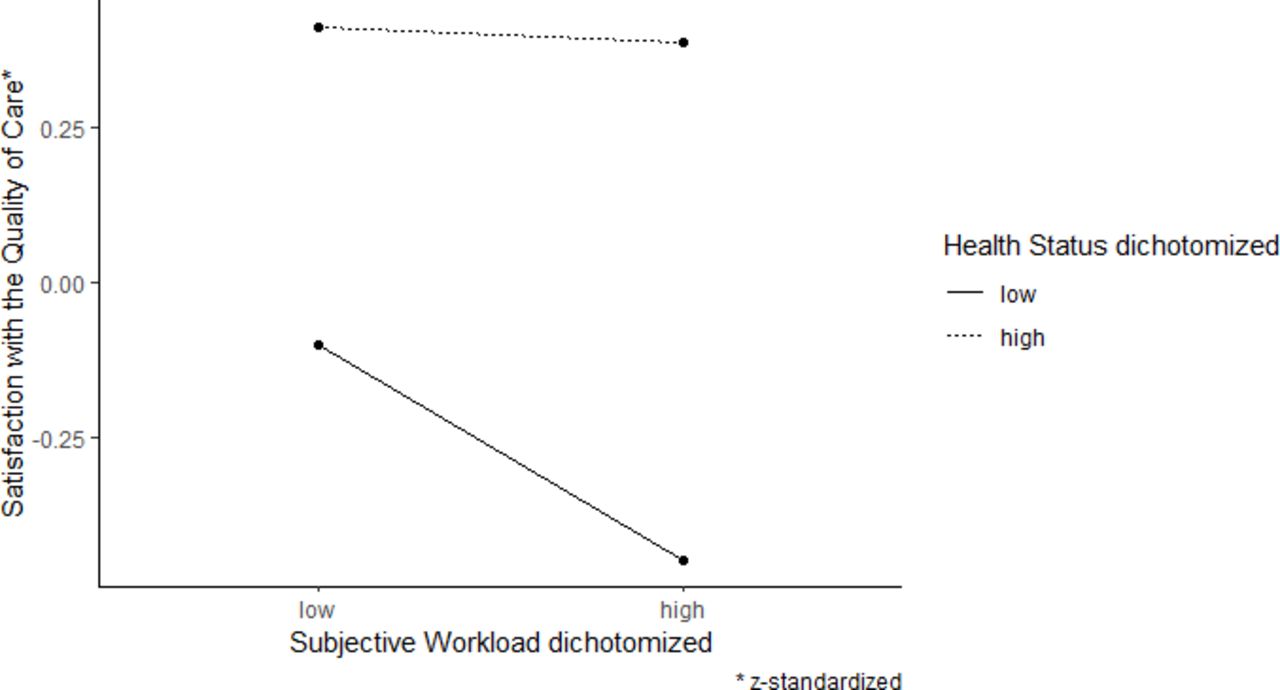
Furthermore, in connection with satisfaction with the quality of care, there was a marginally significant interaction between subjective workload and health status (cf. appendix 7 and figure 1). This interaction was deconstructed by dichotomising the health status variable and computing separate multilevel models. These models included the predictors of subjective workload and organisational commitment as before but excluded effects related to health status. These analyses showed that for nurses who tended to rate their health status as low, subjective workload correlated significantly with the assessment of the quality of care (β=−0.20, t(186)=−2.61, p=0.01). Subjective workload did not show a significant correlation with the assessed quality of care among nurses who tended to assess their health as good (β=0.01, t(123)=0.12, p=0.90).

{kind=link}
Interaction of subjective workload and health status in relation to the satisfaction with quality of care.
Summary of results
Hypothesis 1, a positive correlation between job demands and strain in the form of stress and burn-out, was confirmed by the significant correlations found. The negative correlation of job demands with nurses’ satisfaction specified in hypothesis 2 was shown for job satisfaction and satisfaction with the quality of care. Hypothesis 3, that organisational commitment reduces the correlation between job demands and strain, could not be confirmed due to the non-significant interaction term for stress and burn-out. Only direct negative correlations were found. The positive relation between organisational commitment and nurses' satisfaction, specified in hypothesis 4, could be confirmed for the job satisfaction of nurses and satisfaction with the quality of care. The variable health status directly correlated with all outcome variables examined. Moreover, the correlation between job demands and satisfaction with the quality of care specified in hypothesis 2 was moderated by this variable. The consideration of the work area only contributed to the variance explanation in connection with satisfaction with the quality of care.
Discussion
The significant correlations of subjective workload with all recorded outcome variables showed that job demands at the patient’s bed influence nurses’ everyday working lives, which is consistent with previous findings in Germany.23 24 26 The valences of the correlations indicated that a high workload was related to an increased perception of stress at the workplace and burn-out, which supports previous findings.7 24 41 However, the buffering effect of organisational commitment on this association was not shown. Thus, the assumption of the JD-R that this resource is used to cope with stressors was not confirmed in this context.22 Additionally, organisational commitment showed a possible floor effect, which could indicate that nurses perceived little or no organisational support, which could have affected the relationship between stress and strain, eventually explaining contrary findings to existing research in Germany.26 42
As expected, high job demands were associated with a decrease in job satisfaction and satisfaction with the quality of care which is in line with previous findings. The evaluation of working conditions can differ based on job satisfaction, which could also be a possible relationship in the present survey.43
The positive correlations of organisational commitment with job satisfaction and satisfaction with the quality of care corresponded to the established hypotheses and confirmed previous findings regarding organisational resources.18 44 45 Thus, the direct correlations of organisational commitment with all recorded outcome variables highlight the importance of organisational factors for nurses’ well-being at their workplace, which can also be found in previous research.18 26 42 However, it should be noted that the study design does not allow to derive causality. Notably, only a single resource was considered in this study, and according to the definition of the resources used in the JD-R, the supporting effect can result from the ‘physical, psychological, social and organisational working conditions’.46 This definition shows the variety of existing resources that can influence the experience of job demands and the related strains.
Furthermore, the variable health status was queried because we suspected that it could influence the perception of job demands, strains and satisfaction. No hypotheses have been formulated regarding this variable because no comparable studies with nurses are available. In this analysis, health status was also included in the models as a predictor following the categorisation as a resource.40 Health status substantially contributed to the variance explained in the case of all outcome variables, but especially in connection with burn-out and stress. Further studies are necessary to determine causality and the reason that the interaction of the subjective workload and health status only occurred in connection with the quality of care.
The controversial findings on differences among work areas are based on the specifics of the working conditions and the different job demands and strains that accompany them,28 which led to inclusion in this study. In the conducted analyses, the consideration of the work area only led to an improvement in the model with the outcome quality of care. This finding suggests that there are no significant differences between the domains when considering the other outcome variables. This result supports previous research that found no difference between general and intensive care staff.47 Because the present survey focused exclusively on nursing activities in connection with the patient’s bed, we should consider that these specific demands occur equally in all surveyed areas.
Limitations
The questionnaire only captured the workload connected to the patient’s bed, as the study focused on this specific work area. Thus, this is only a fraction of the existing job demands of nurses, which becomes evident when referring to the definition of nursing workload.10 The definition explicitly lists nonpatient-related activities or the amount of time that nurses must spend on care activities. The latter was also queried in this study in connection with the nursing activities but was not tested in the form of hypotheses because of a lack of comparable studies. Additionally, this scale was included to allow comparison with future surveys.
To ensure the anonymity of the participants, no detailed differentiation of the wards was possible. Thus, the results could not be related to the individual circumstances of the wards, such as the patient-to-nurse ratio or the sickness rate of staff, which could have provided further insights. Due to the convenience sampling approach, a sample bias cannot be excluded. Considering the sample description (cf. online supplemental appendix 1) we did not see any systematic effects leading to a non-response bias of certain groups. The gender distribution of participants is comparable with the overall gender distribution of German nurses with 83% female and 17% male nurses.48 Regarding the age distribution, we observed a slight overrepresentation of nurses in the age group of 25–34 years and an under-representation of nurses being 45 and older, compared with the population of nurses in Germany.49 Nevertheless, we think the results on stress and strain of nurses can be compared with studies using other sampling methods, which is supported by similar findings in existing literature. Though the sample was not randomly selected and was limited to one clinic the results found should not be generalised and further research in other hospitals is necessary to draw conclusions about all nursing professionals.50
Furthermore, it should be noted that data collection took place during the initial phase of the COVID-19 pandemic, which could have affected the nurses’ answers. The response rate being within the usual scope of comparable surveys in similar populations, thus its admittedly low value could be just due to the high workload of the nurses.24 26 The proportion of missing values was still acceptable.51 The answer option ‘not applicable’ also attempted to limit non-response error, thus it cannot be ruled out completely.
Conclusion
Based on the results, initial measures of action that can benefit nursing staff can be derived. The strong correlations found between organisational commitment and subjective workload with strain and satisfaction are of particular importance. With the correlations found, projects should be developed to improve the work area of the patient’s bed, such as introducing technologies that assist nurses in their routine work. Additionally, investigations should be conducted on how the organisation can support nurses better. Because the overall organisational commitment has a low rating, the strong correlation of health status with all variables studied can provide a starting point for organisational measures. Through an expansion of occupational health management, a positive influence on the health of employees could be exerted, and the perception of organisational commitment could be improved.
Supporting nurses at their central workplace and taking measures of improvement provides the opportunity to value nursing as a highly relevant professional group and to improve its working conditions and the quality of patient care.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the ethics committee of the university clinic Göttingen reviewed the questionnaire and approved the study project (file number 11/1/20). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MGF and MB are joint senior authors.
Twitter @KWenderott
MGF and MB contributed equally.
Correction notice This article has been corrected since it first published. Under key message box, "How this study might affect research, practice or policy" section has been updated.
Contributors The empirical research of this study has been conducted as a master thesis project by KW. KW, therefore, contributed to the development of the questionnaire, the statistical analyses, the interpretation of the findings, and writing of the manuscript. SF contributed to the development of the questionnaire, the implementation at the university medical centre, management processes and writing of the manuscript. MGF contributed to the overall design of the study, management processes and writing of the manuscript. MB contributed to the supervision during the development and implementation of the questionnaire and the writing of the manuscript. MGF and MB contributed equally to this study, they share the senior authorship and act as guarantors of the study.
Funding There has been financial support for organisational purposes to conduct this study from ABLY Medical AS, but neither financial benefits for the authors nor influence on its outcome was taken. No award/grant number.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.